Infectious Diseases Case of the Month Case #34 |
|||
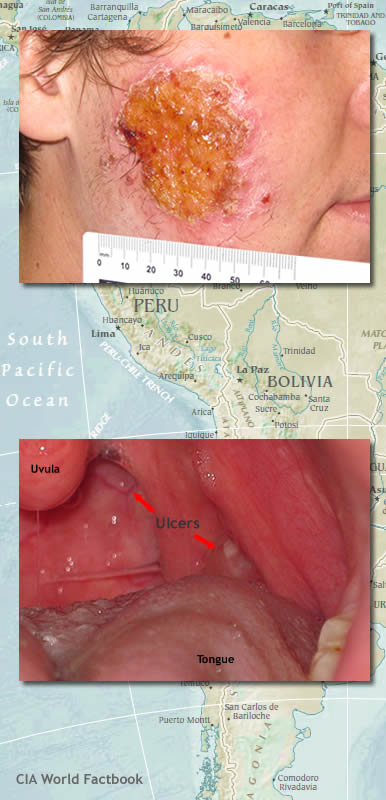 |
A twenty three year old white male was seen in infectious diseases clinic in April 2011 for a large facial sore and a sore throat. He had recently returned from a five to six month stay in South America where he and his fiancé had visited multiple countries in a combined adventure/work experience. He began his odyssey in October 2010 in Ecuador including a visit to the Galapagos. In late November he proceeded to the Amazon region of Peru. While his fiancé studied macaws as part of a research project, he did filming for local resorts for the production of promotional video. On one occasion in early January 2011 while filming in a remote area along the Heath River (which forms a portion of the Peru-Bolivia border), he recalled in particular numerous bug bites, primarily on his lower extremities, but likely elsewhere as well. He and his fiancé then proceeded on to Cochabamba, Bolivia for the next two months of their sojourn. There he continued working on video projects as well as participated in volunteer work including installation of solar panels and assisting disadvantaged children. It was while in Bolivia in February 2011 that he first noticed a small "pimple" on his right cheek. This slowly and progressively enlarged and ulcerated such that by March it had become an relatively large open ulceration. He saw a physician in La Paz who administered an intramuscular antibiotic and prescribed an oral antibiotic and topical anti-fungal cream. He returned to the United States in late March and sought care from his primary care physician. He was prescribed ciprofloxacin and ampicillin/clavulanate without apparent benefit. He was referred to a dermatologist who performed a skin biopsy, and he was thereupon referred for infectious diseases consultation. In mid-late April shortly before being seen in the ID clinic he had also developed sores on his pharynx (see lower left). His facial lesion at that time had become quite large (see upper left) although it remained painless. He was previously healthy, and at the time of his ID evaluation routine laboratory data including CBC and comprehensive metabolic panel were normal. An HIV antibody was negative. He was referred to an ENT physician for biopsy of the pharyngeal lesions. |
||
What is the most likely insect vector of this disease? |
|||
 |
Biopsies of both the facial and pharyngeal lesions showed the amastigotes of Leishmania braziliensis (as identified at the CDC), an organism transmitted by sandflies. Pictured at left are the five insects from the previous vignette, all of medical significance. The top four (sandfly, louse, triatomine bug, and mosquito) are vectors of human disease while the botfly (Dermatobia hominis) is a cause of myiasis. The four vector insects are all hematophagous in some aspect of their life cycle, and in the process of acquiring a blood meal may transmit infection to humans. Found mainly in the tropics and subtropics, there are over seven hundred species of sandflies, perhaps seventy of which are involved in transmission of disease to humans (leishmania, viruses, and bacteria (Bartonella bacilliformis)). Sandflies inhabit a wide range of habitats from hot dry deserts to dense tropical rainforests. They are very small (1.5 - 3.5 mm) and are distinguished from other small Diptera (true flies) by how they hold their wings above their body like a vertical "V" (see topmost image at left). They are weak fliers and usually only fly at night though if disturbed during the day, they will also be active and bite. At least thirty species of sandflies transmit leishmania to humans. Avoiding exposure can be difficult as their very small size allows sandflies to penetrate standard sized screens and mosquito nets. Fine sandfly bed-nets can be protective, but these can be uncomfortable to sleep under in humid tropical climates. Insect repellents (DEET, etc), used appropriately, can effectively repel these insects. Human body lice (image #2 at left) are vectors of epidemic typhus, trench fever, and louse-borne relapsing fever. Body lice live on clothing and bedding used by infested persons. Body lice must feed on blood and usually only move to the skin to feed. In the United States, body lice infestations are found only in homeless transient populations who do not have access to bathing and regular changes of clean clothes. Triatomine bugs ("kissing bugs"- image #3 at left) are vectors of South American trypanosomiasis (Chaga's Disease). Both sexes of these bugs feed solely on vertebrate blood, and thus their primary habitats are in or near the burrows of a variety of wild animals. A number of triatomine species have the ability to colonize the crevice habitat of simple mud and wattle or unplastered adobe brick Latin American homes from which they can conveniently feed on humans. Mosquitoes (Aedes aegypti is pictured - image #4 at left) are vectors of numerous human diseases some of extraordinary historical and contemporary significance. Diseases include malaria, filariasis, yellow fever, dengue fever, and numerous other arboviruses. There are more than three thousand described species of mosquito inhabiting a very cosmopolitan range from the tropics to the arctic. Most but not all mosquito species hunt and feed at night and have well defined activity cycles (some attack at dusk, others at midnight, etc). Larvae of Dermatobia hominis (lowermost image at left) are "ingenious" hitchhiker causes of human and veterinary myiasis. A case of myiasis was featured in Case of the Month #20. Click here to learn more of this very interesting illness. The case of leishmaniasis featured in the preceding vignette was very unusual in the early development of mucocutaneous disease. Mucocutaneous leishmaniasis is a potentially disfiguring complication of cutaneous leishmaniasis whose onset is usually months to years after the primary cutaneous disease, often after apparent resolution of the skin disease. For more details of leishmaniasis see Case of the Month #30.
Ref: Manson's Tropical Diseases, 21st ed, Elsevier, 2003 |
||
| Home Case of the Month ID Case Archive | Your Comments/Feedback | ||